Mixed messages
All types of communications arrive in a single inbox without clear differentiation.
AI-assisted triage for community-based clinics. FlowMD reads incoming messages and suggests routing, urgency, and missing information — so your team stops sorting and starts caring.
Built for Ontario clinics. Designed around OMD-certified EMRs.
Suggestions only — your team always decides.
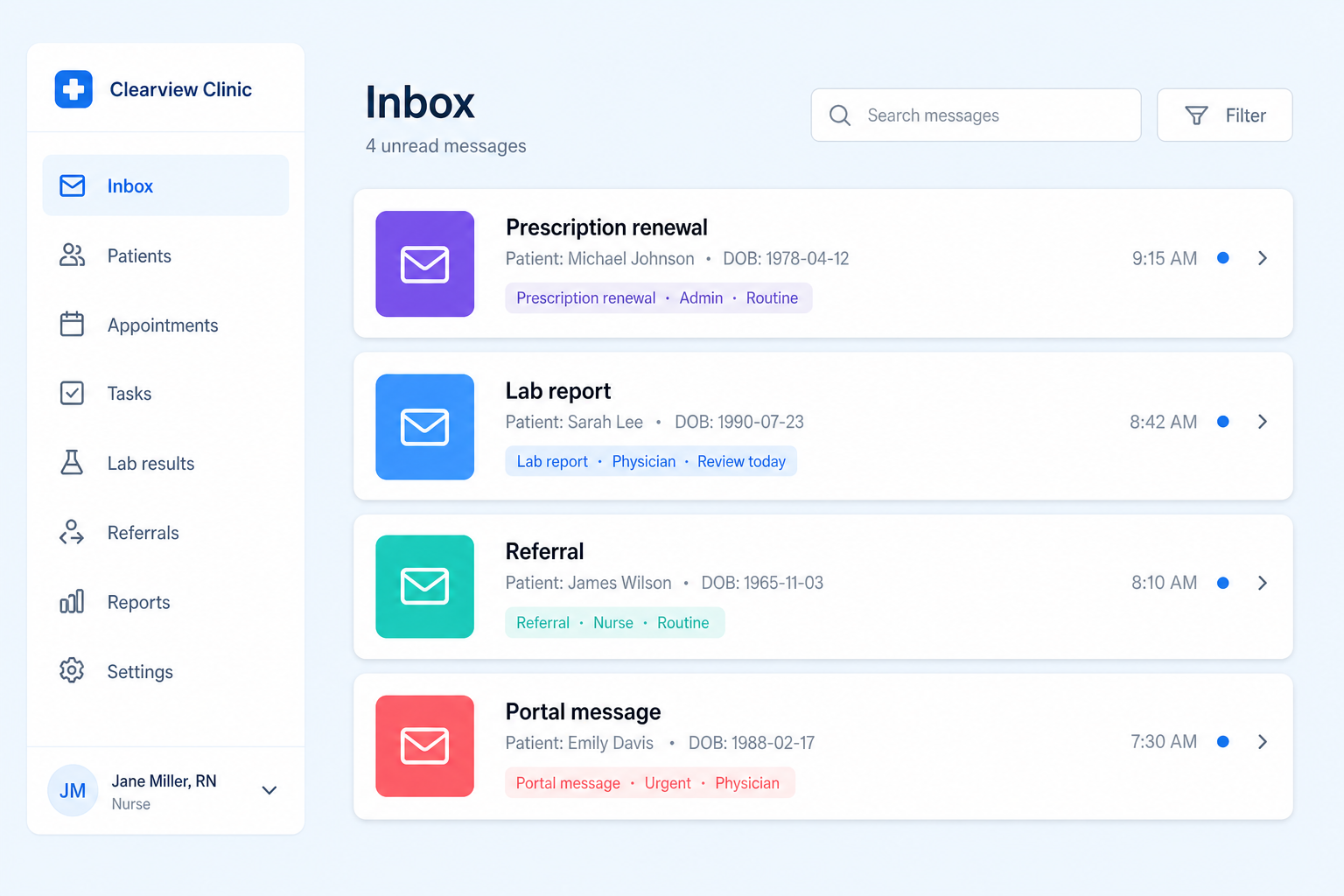
Community clinics receive a constant stream of prescription renewals, referrals, lab reports, portal messages, and administrative forms. Most EMRs are passive repositories — every message has to be read, categorised, and routed before any care decision begins. The cost isn't the volume. It's the constant interruption.
All types of communications arrive in a single inbox without clear differentiation.
Urgent and routine requests look identical at first glance.
Staff must read and categorise every message before real work begins.
Highly trained clinical staff spend valuable time triaging instead of helping patients.
FlowMD reads each incoming message and adds four pieces of context — before your team opens it.
System indicates whether the message is best handled by physician, nurse, or administrative staff.
Messages receive a suggested priority level based on content and clinical context.
Each suggestion includes a brief explanation of why it was classified that way.
Team members review suggestions and make final routing decisions, with full override capability.
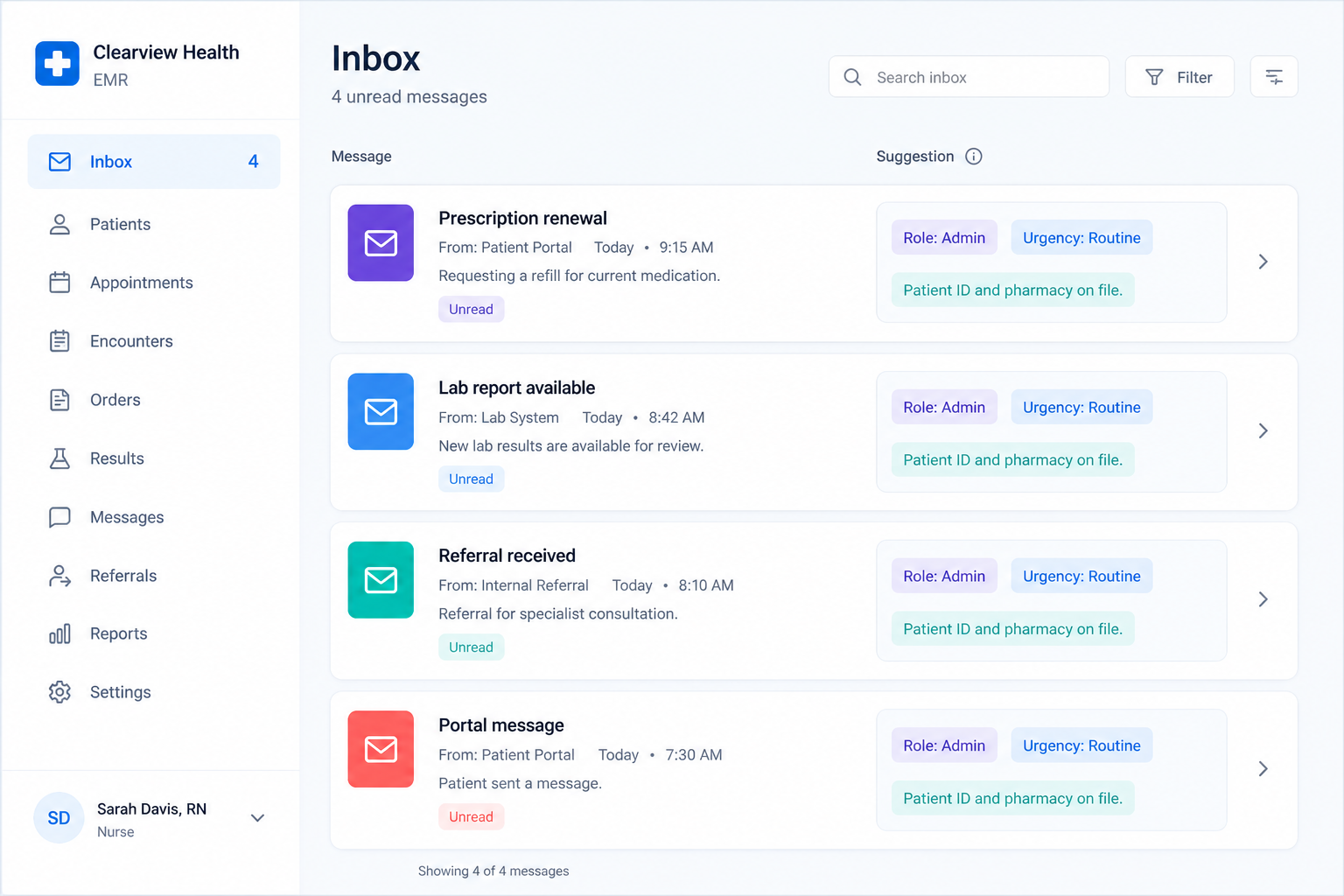
FlowMD layers on top of your existing inbox. Your team sees the same messages they see today — with a small panel of suggestions next to each one.
| Today | With FlowMD |
|---|---|
| Single inbox with mixed content | Same inbox, enhanced with suggestions |
| No visible urgency indicators | Suggested role and urgency level |
| Manual triage required | Brief explanation for each suggestion |
| Staff determines routing independently | Staff reviews and decides final action |
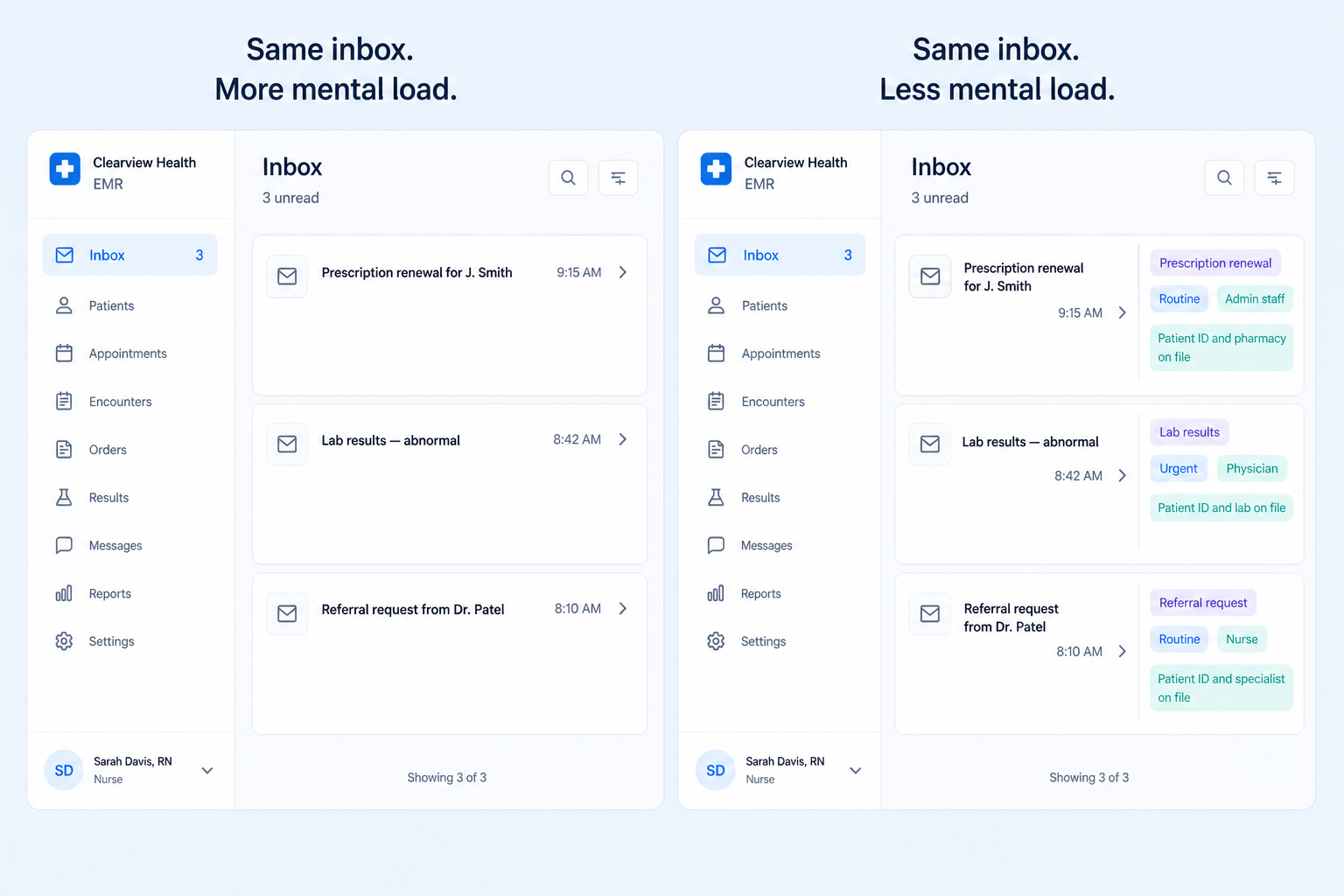
FlowMD connects to your existing channels. Your team's day doesn't change — it just starts with more context.
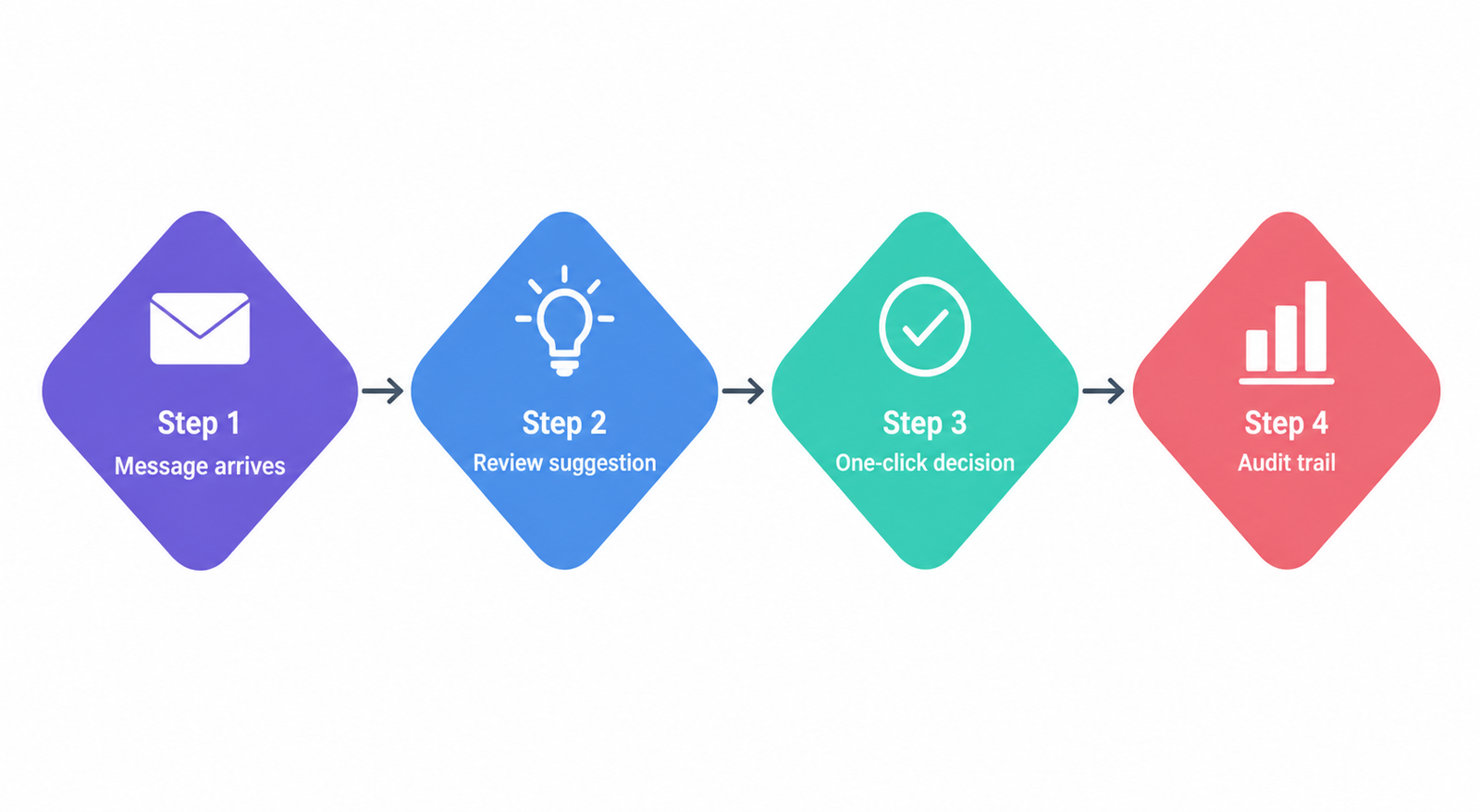
Communications continue to arrive through your existing channels without disruption.
Staff see suggested routing and urgency alongside the message content.
Accept the suggestion, or override with your own judgment. One click either way.
Clear documentation of every decision, for quality assurance and ongoing learning.
We test FlowMD's accuracy against representative inbound data from your clinic. No live workflow changes.
Clinic lead + FlowMD team
FlowMD runs alongside your current process. Every suggestion requires human confirmation. We measure accuracy and time saved.
Triage staff, with weekly check-ins
FlowMD integrates with your OMD-certified EMR. The team uses it daily, with full override and audit visibility.
Whole clinic
The goal is workflow optimisation, not diagnostic automation. We move to the next phase only when your team is ready.
How often FlowMD's suggestion matches what your team would have chosen. Preliminary experiments: 90–95%.
How often staff accept a suggestion without override. The gap is where we improve.
Average minutes from message arrival to routed action, measured before and after FlowMD.
Surveyed at baseline, mid-pilot, and end. Both clinical and administrative staff.
FlowMD is built to operate within Ontario's Personal Health Information Protection Act (PHIPA) framework. Data handling, retention, and access logging follow PHIPA principles. Hosting on Canadian infrastructure with no cross-border data transfer in default configuration.
FlowMD never sends, replies, files, or routes on its own. Every action requires a human decision. The system is assistive — it does not practise medicine, does not make diagnostic determinations, and does not replace clinical judgment.
Every suggestion FlowMD makes, every override, and every accepted decision is logged. Your clinic owns the data. You can export, review, and delete at any time.
FlowMD is designed to integrate with OMD-certified EMRs. Certification work is in progress; we'll publish status as it advances.
FlowMD is built for the daily reality of family medicine and community practice in Ontario. If any of these sound like your clinic, the pilot is for you.

We're working with a small group of Ontario clinics through 2026. If you're interested in being part of the pilot cohort, tell us a little about your practice and we'll be in touch within two business days.
Data stays in Canada. PHIPA-aligned from day one.
That's all we ask of your team during the pilot.
Export your data and leave whenever you choose. No lock-in.
Thanks — we received your application. We'll be in touch within two business days.